







 Official publication of the Czech Society of Ultrasound in Obstetrics and Gynecology.
Official publication of the Czech Society of Ultrasound in Obstetrics and Gynecology.



Introduction: This study was conducted to determine the occupational burnout and its dimensions in Babol hospital personnel, as well as determining the levels of work, social support and self-esteem in these staffs.
Methods: In this study, demographic information questionnaire was distributed internally among 130 hospital personnel. Maslach Burnout Inventory (MBI) was used to measure the severity of occupational burnout. In the Maslach inventory, the frequency of the studied units in each of the occupational burnout dimensions including: emotional exhaustion, personality depersonalization and decrease in personal adequacy with a Likert scale in a low-medium and high-grade manner were evaluated and data analysis was performed by SPSS 21 software and descriptive-analytic tests.
Findings: Regarding the dimensions of occupational burnout, the findings indicated that the mean of personal adequacy was 31.78 ± 8.726 out of the total score of 48, the mean of emotional exhaustion in the employees was 26.53 ± 12.624 out of the total score of 54 and the mean of the personality depersonalization was 5.70 ± 5.444 out of the total score of 30. Personality adequacy was low in 43.8 % of employees, emotional exhaustion was high in 47.7 % of people and personality depersonalization was low in 69.2 % of people. There was a significant correlation between occupational burnout dimensions and variables of gender, work history, marital status, place of employment, occupation and work experience of staff (p < 0.05), the rate of workload with emotional exhaustion (p = 0.000 and r = -0.608) and personality depersonalization (p = 0.000 and r = -0.357) showed a significant and inverse correlation.
Conclusion: The total amount of occupational burnout in the staff was related to emotional exhaustion (moderate), personality depersonalization (low) and personal adequacy (low).
Occupational burnout can be defined by analyzing the psychological powers that sometimes come with depression and trying to help mental patients or people under stress (1). The characterized burnout by a set of symptoms that includes exhaustion resulting from work’s excessive demands as well as physical symptoms such as headaches and sleeplessness, quickness to anger and closed thinking. Occupational burnout Excessive fatigue syndrome is followed by years of conflict and commitment to work and people. In other words, the occupational burnout is physical, emotional and psychological fatigue in a long-term problem in difficult job (2). This syndrome is a condition in which the strength and ability of people with low desire and willingness to work and activity decreases (3). Occupational burnout is a consequence of continuous and frequent job pressures. In this way, the person in the workplace is pressured by internal and external factors, and this pressure is continuous and repeated, and eventually becomes a burning sensation. Occupational burnout is defined as a lack of energy and vitality, and a person with burnout shows a calmer feeling of doing business behavior. A person who has synergistic responsibilities will have the feeling that it will be drawn in several directions. This will result in fatigue and, ultimately, occupational burnout. The first occupational burnout injury is suffering from burnout, such as headache, nausea, short sleep, and changes in food habits. Emotional exhaustion such as depression, feelings of helplessness, feeling of inefficiency in your job, as well as negative attitudes towards yourself, your job, your organization, and overall life-threatening outcomes are occupational burnout. Occupational burnout is a deterrent to the creation and expansion of job satisfaction (4). This syndrome has many effects on the individual’s social, physical and psychological life. Medical staff due to stress such as mortality, interpersonal problems, low social support, high workload, exposure to a large number of patients per day (5-9), emergency decision making based on inadequate and responsive information being in touch with the results of this decision, stress-struggling efforts to avoid any mistake, exposure to violence and workplace threats are more likely to be involved in the syndrome than other businesses (10-13).
In many cases, stress and occupational burnout cause absenteeism and wasteful working days. Cox writes about this: It is estimated that an average of 37 million daily jobs are wasted due to mental disorders, neurological disorders, headaches and worn out all emotions and emotional feelings are lost to the clients, and in some cases, they provide care inappropriately and inanimately (11). Nurses who experience occupational stress often experience unpleasant distress, fatigue, lack of tolerance, hardship with patients and their families, avoiding colleagues, anger and, generally speaking, unbearable for their colleagues (12-13).
In a survey conducted by Moghiman, the results showed that the average wage score in the research units was 48.95 ± 13.83 and 78.2 % of the subjects were occupied in the moderate score occupational burnout (14).
Gillespie and his colleagues randomly studied 510 Scottish nurses in Maslach’s inventory to survey occupational burnout of nursing in psychiatric nurses. Respondents showed moderate, low and moderate levels of emotional exhaustion, depersonalization and personal adequacy (15).
The results of Esfandiari’s research also showed that 2.9 % of the nursing staff had occupational burnout (16). In the Kluger study, 20 % of the population showed high emotional exhaustion, 20 % high personality depersonalization, and 36 % low personal adequacy. Only 1.4 % suffered from occupational burnout syndrome (17).
In the Rosdahl study was conducted on the measurement of occupational burnout and job satisfaction in nurses of the bone marrow transplantation department in Liverpool. The results showed that: 10 % of the units reported high levels, 52.5 % of the moderate levels and 37.5 % of the lower levels of emotional exhaustion (18).
Hospital personnel are among those who are in close contact with other people and are responsible for the health and life of humans and exposure to a negligent person with acute and chronic illnesses, since occupational burnout affects the quality of care of the client, more effective identification of the factors affecting the quality of the services offered in the field of health and treatment will be useful. On the other hand, most of the studies on occupational burnout have been done on the health personnel and there is not much information about occupational burnout in health personnel. Therefore, we decided to investigate the frequency of occupational burnout and related factors among Babol hospital personnel to plan and compare with other regions of the country, as well as comparisons with other countries.
The present study is a descriptive-analytic study that aimed to investigate the occupation dimensions of hospital staff among Ayatollah Rouhani hospital personnel of Babol includes nurses and administrative staff and nurse aid in 2017 using simple random sampling method and using Cochran formula at 5 % error level, the personnel employed in the hospitals (except doctors) were determined in three shifts of morning, noon and night of 130 people who were randomly assigned to the study Accordingly, 130 questionnaires were distributed among the personnel and all 130 questionnaires were completely completed and returned. Due to the sensitivity and dynamics of hospital occupations and the lack of time to fill the questionnaire, in order to increase the accuracy of the data, the researcher has been involved in facilitating the transmission of the concept of questions when completing each questionnaire. Therefore, the process of distributing and collecting questionnaires with a high accuracy and distribution time, taking into account shifts, lasted two weeks.
To collect data, a questionnaire containing two categories of questions related to individual characteristics as well as Maslach occupational burnout inventory, which includes 22 questions and 3 scales of occupational burnout (emotional exhaustion - personality depersonalization- personal adequacy), are evaluated in terms of frequency. 9 dimensions about emotional exhaustion, 5 dimensions about depersonalization, and 8 dimensions about personal adequacy. The frequency of these emotions is measured by scores from zero (never) to six (every day) and a separate score is obtained for each aspect. The validity and reliability of the Maslach occupational burnout inventory for the first time in Iran was confirmed by Philian. He used a re-test method to determine scientific reliability and the results of both stages were calculated using the correlation test. The final findings showed a strong correlation between the responses given in two stages of the test and equal to 0.98 (19).
The content validity method was used to determine the validity of the demographic questionnaire. In this way, following the study of new scientific articles on this subject, of under the supervision of the relevant faculty, and after considering the correctional views of several experts, the validity of the questionnaire was supported. To determine the reliability of this tool, a test-retest method was used. First, this form was completed for 15 eligible individuals and was repeated again within one week. Then, using Pearson correlation coefficient, the reliability of the tool was confirmed with r = 1. The data were analyzed by SPSS version 21 and analyzed by descriptive statistics such as percentages and ANOVA and Tukey post hoc test, Pearson correlation coefficient and independent t-test.
It should be noted that in the distribution of the questionnaire, the sample population was assured that the questionnaire was designed without mentioning the name and the relevant section and with the assurance of the nurses and management of the hospital, data analysis was carried out. Also, based on research ethics, the researcher has applied caution to increasing the accuracy of data collection and analysis.
130 hospital staff completed questionnaires. 23.8 % of the samples were nurses, 56.9 % of the administrative staff and 19.2 % of the nurse aid were selected. The results showed that 30.8 % of the research subjects and 69.2 % of women and the average work experience in them were 13.84 ± 6.913. In terms of marital status: 7.7 % were single, 92.3 % were married. In terms of education: 30 % had an undergraduate degree, 49.2 % had a bachelor’s degree, and 20.8 % had a master’s degree. In terms of employment status: 63.8 % of the official personnel, 18.5 % of the contract, 6.9 % of the plan, and 10.8 % of the other cases (pseudo-contractual agreement). The age range of the units under study was in the range of 23 to 58 years old and the mean age of the subjects was 38.88 ± 8.0005. Regarding the dimensions of occupational burnout, the findings indicated that the mean of personal adequacy was 31.78 ± 8.726 out of the total score of 48, the mean of emotional exhaustion in the employees was 26.53 ± 12.624 out of the total score of 54 and the mean of the personality depersonalization was 5.70 ± 5.444 out of the total score of 30 (Graph 1).
Graph 1 Occupational burnout dimensions of hospital staff
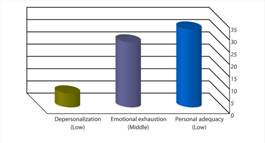
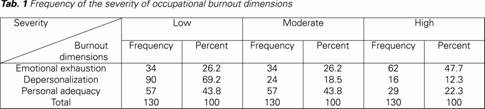
In other words, considering the cut lines of the Maslach inventory, the subjects studied the occupational burnout in the staff was related to personality depersonalization (low), emotional exhaustion (moderate), and personal adequacy (low). The findings also showed that personal adequacy was low in 43.8 % of employees, 47.7 % in terms of emotional exhaustion in high level and the level of personality depersonalization was 69.2 % in low level (Tab. 1).
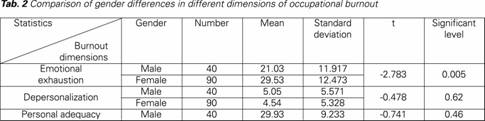
The mean of personal adequacy and emotional exhaustion in females is higher than males and the average depersonalization rate in males is higher than that of females. There is a statistically significant difference between gender and emotional exhaustion, so that the mean of emotional exhaustion in females is higher than males (P < 0.005).
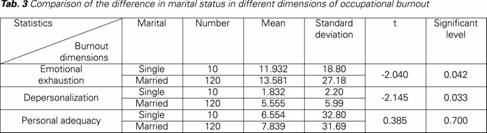
T-test showed that the occupational burnout mean rate in the dimensions of depersonalization and emotional exhaustion in married people was significantly higher than single subjects (P < 0.05)
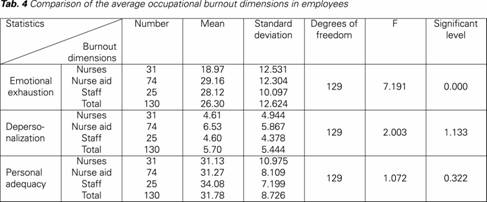
ANOVA test showed that there is not a significant relationship between occupational burnout and educational level (P > 0.05). The results indicate that the average of personal adequacy in official staff is higher than other employees. ANOVA test showed that there is not a significant statistical relationship between occupational burnout and employment status of employees (P > 0.05). The findings showed that the average of personal adequacy in nurses was higher than other staff. The mean of emotional exhaustion in the administrative staff and the average person depersonalization in nurse aid health care workers is higher than other employees. ANOVA test shows that there is a statistically significant difference between job type and occupational burnout in emotional exhaustion ( Tab. 4).
In this research, 47.7 % of the employees have estimated the frequency of emotional exhaustion at a high level, which is consistent with the results of Caballero et al.’s research on the existence of severe emotional exhaustion in 30.6 % of nurses and on the other hand, it can indicate the undesirable situation of the personnel studied in this research. Experts say moderate to severe levels of emotional exhaustion can be due to conflict of role and defect, excessive duties, interpersonal and interpersonal conflicts. Researchers believe that feeling emotional exhaustion reduces the psychological ability of an individual, so that he or she experiences a kind of cold with excessive indifference to the client and the profession. Therefore, it can be concluded that most employees probably cannot prove their competencies in the workplace, and this can be due to the absence of positive conditions in the workplace (21).
The findings of this study revealed low levels of personal adequacy in most of the research units that did not match the findings of Yaghoobnia and Robert (1,20). The feeling of success and mastery is created when a person can influence the policies of the organization and thereby display his abilities and gain a positive attitude toward himself and the client. The findings also showed that the majority of research units in the depersonalization dimension were low, which is consistent with Gillespie’s and Robert findings in this regard (15,20).
The findings of the present study also showed that the mean score of emotional exhaustion was 26.52 out of a total score of 54 which is classified in the middle class of Maslach. These results are consistent with Yaghoobinia’s findings (1). In this study, the mean of emotional exhaustion is relatively high in comparison to similar studies, which can be considered and can seriously interfere with the role and duties of these personnel. The reason for this can be several issues, such as high work pressure, tedious work environment, high stress in the workplace, low salaries and benefits, and overlapping of tasks in the workplace. It is possible to reduce the fatigue of these people by reducing the hours of work, as well as adding the recreational programs of the employees. Nowadays, the program of reducing the working hours of nurses in the country is running, and how good is it to be implemented by keeping track of the authorities, reducing the hours of work for health personnel and see more productivity in working environments for this massive and hardworking country that is actually at the front of the country’s health front.
In this study, the average personal depersonalization was 5.70 % of the total score of 30, which is located on the lower level. These results are consistent with Yaghoobnia´s findings (1). Personal depersonalization is defined as the psychological separation of a person from his job and as a result of a negative reaction to feelings, combined with excessive neglect of service recipients (4). In the present study, the average of personal adequacy score of the employees was 31.78 out of a total score of 48, which is placed on the bottom (risk factor). The results are based on the findings of the findings of Philian (19), Talaei (22), Momeni (23), Yaghoobnia (1), Kluger (17), Rosdahl (18), Dick (24) and Robert (20) is consistent in personal adequacy. The high level of occupational burnout in the aspect of inadequacy of the personal adequacy can indicate a negative attitude towards themselves and their careers, and a lack of interest, satisfaction with the job, and lower self-esteem in individuals (16).
In this study, the occupational burnout dimensions in hospital staff were low in emotional exhaustion and depersonalization in middle and low level and in personal adequacy. In other words, these employees were at risk in terms of occupational burnout and its three dimensions in terms of emotional exhaustion and inadequate personality. These results are consistent with Janson’s findings (25). On the other hand, Yaghoobnia, Moghiman, Dick, and Kilfedder have reported average occupational burnout alert levels in the research units (1,14,24,26).
Potter has recommended adopts moderator and preventive measures in people who have low levels of occupational dysfunction, extending programs that modify problematic areas for people with moderate levels of occupational dysfunction, and finally take corrective action for those who high levels of occupational hangover (27). Persons with high expectations and motivation, ideals and hope are very likely to enter the work environment and are working under conditions that are high in the care needs of the clients, are prone to occupational burnout (21).
The findings showed that there is a significant statistical relationship between gender and occupational burnout dimensions, so that women report higher personal qualities and emotional exhaustion than men. On the other hand, women have more personality depersonalization than men. Kilfedder reported that there is no meaningful statistical relationship between gender and occupational burnout dimensions (26). Findings of Philian showed that there is a significant statistical relationship between gender and emotional exhaustion, and the level of emotional exhaustion in males was more than that of females (19).
The findings also showed that the age of the employees with occupational burnout was not statistically significant, with the findings of Ozyurt (28), Alavi (29), Bellani (32), Kilfedder (26), Boyle (33), Sahraian (31) is inconsistent in this regard and, on the other hand, is consistent with the findings of Moghiman (14), Mirab-Zadeh (34) and Abdi (30).
In this study, the relationship between marital status and occupational burnout dimensions was statistically significant, which was not consistent with the findings of the Mirab-Zadeh and Taee (34-35), and is consistent with the findings of Moghiman, Talaei, and Philian in terms of depersonalization and emotional exhaustion (14,19,22).
In this study, the history of work experience of staff with occupational burnout dimensions was statistically significant, which is not consistent with the findings of the Mirab-Zadeh and Taee (34-35), and on the other hand, Esfandiari and Moghiman’s findings have been consistent with the variables of the work (14,16), and are consistent with the findings of Moghiman, Philian and Talaei, in terms of depersonalization and emotional exhaustion (14,19,22). Also, the results of the study showed that the average occupancy rate of people with high work experience is lower than those with low work experience. Increasing employee experience seems to be associated with increasing occupational burnout
The results of this study showed that, given the high levels of emotional exhaustion and personal skills reduction, and the proven role of occupational burnout in reducing staffing efficiency, more attention from the authorities and practitioners to improving and improving the conditions in the workplace is recommended. Respecting employees’ point of view and their actions and their views, as far as possible by the authorities, can improve their efficiency and reduce occupational burnout.
Experience shows that counseling centers for hospital staff, rehab health education and mind control can be effective. Also, the study of the experiences of successful hospitals of other countries in controlling the above components can be inspirational so that localization and creation of capabilities and capacities in the country can benefit from their positive results. The generalizability and support of the findings of this study is possible through conducting qualitative research. The application of the findings of this study and the proposed studies can help hospital managers to create ethical workplace environments and promote ethical care, thus reinvigorating the positive characteristics of hospital staff and creating a supportive environment for them.
It is suggested that future researchers should be encouraged to reduce the stress and increase mental health. Among the practical proposals, the immunization program and the promotion of mental health can be formulated as an in-service training for staff.
One of the limitations of this research is the non-issuance of research results to other organizational categories due to differences in the identity of nursing careers and their functional areas compared to other occupations, and because of community constraints, samples and the use of a tool (a questionnaire) for data collection, it is necessary to be cautious in generalizing the results.

